Female sterilization procedures
An overview of ovariohysterectomy and ovariectomy procedures
This article was updated March 25, 2024.
Surgical sterilization is the most performed procedure in veterinary medicine. Traditional sterilization techniques involve removal of the gonads, which eliminates hormonal secretions in addition to reproductive potential. The most common procedures performed to accomplish this in females include ovariohysterectomy (OVH) and ovariectomy (OVE). Each of these procedures has associated risks and complications.
OVH vs OVE

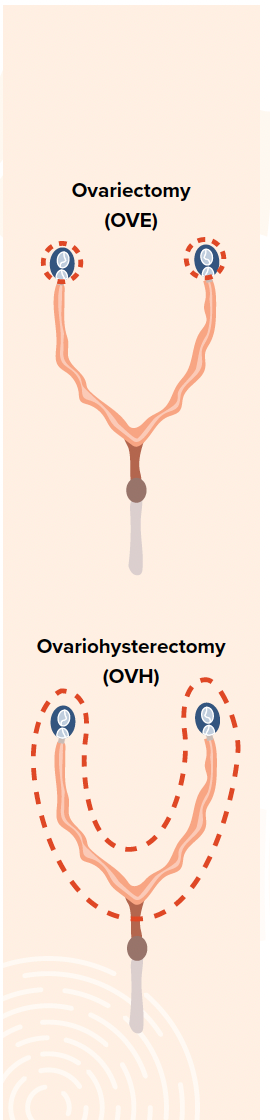
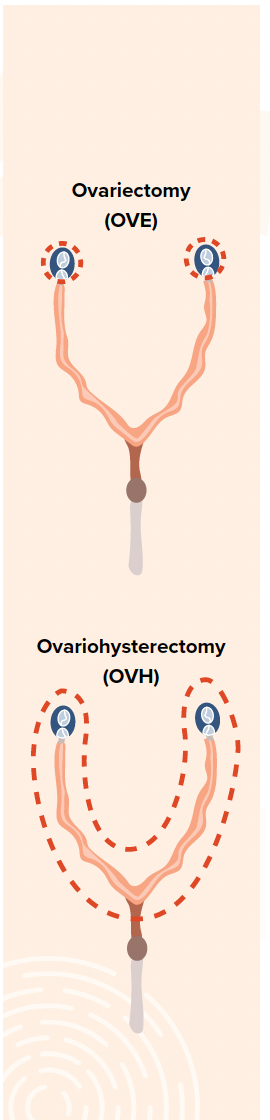
An OVH involves removal of the ovarian and uterine tissues, whereas an OVE involves the removal of ovarian tissue only. Both procedures significantly decrease the risk of uterine and mammary cancer, significantly decrease the risk of pyometra development, and effectively prevent unwanted pregnancy. From a technical standpoint, an OVE is less invasive, requires a smaller surgical incision, is less time consuming, and causes less tissue trauma. Potential advantages of this procedure include improved visualization of the ovarian pedicle, decreased risk of hemorrhage, shorter surgery time, and improved patient recovery.1 Theoretically an OVE is safer and less technically demanding; however, the veterinary literature has not shown a difference in short- or long-term outcomes when compared to OVH.2
The major benefit of an OVH is the ability to remove the uterine tissue along with the ovaries. Therefore, when uterine pathology is present, including congenital uterine abnormalities, pyometra, mucometra, cystic endometrial hyperplasia, uterine torsion, uterine prolapse, uterine rupture, and/or uterine neoplasia, an OVH is preferred over an OVE.
Laparoscopic techniques
In the past decade, there has been an increased interest in minimally invasive surgery using laparoscopic techniques from veterinarians and pet owners. The benefits of laparoscopic approaches have been well established and include decreased surgical and anesthetic times, improved visualization of abdominal organs, a reduction in postoperative pain, decreased surgical stress, and a decreased incidence of wound healing complications.3-5 Typically, an OVE is the most performed surgical technique when laparoscopy is desired; however, an OVH may still be performed using minimally invasive techniques.
A laparoscopic approach typically utilizes 1 to 3 portals to gain access to the abdominal cavity. The abdominal cavity is insufflated with gas, typically carbon dioxide, for improved visualization. Hemostasis is generally achieved with bipolar vessel sealing devices. If an OVH is to be performed, a laparoscopic-assisted approach is used, meaning one of the portal incisions is extended to facilitate removal of the uterine tissue. This results in longer incisions compared with a laparoscopic OVE and may decrease the traditional benefits of a laparoscopic procedure.
Potential complications of laparoscopic procedures include subcutaneous accumulation of carbon dioxide, omental herniation, seroma formation, and/or splenic, ovarian pedicle, or uterine hemorrhage.6 In some cases, conversion to an open abdominal approach is required if visualization is impaired or hemorrhage cannot be controlled. Complication rates are similar between laparoscopic OVE and laparoscopic-assisted OVH procedures; however, laparoscopic OVE has been associated with shorter surgical times, which may decrease overall complication rates.7 Although there are many potential benefits to laparoscopy, the technique is often more costly, requiring advanced training and specialized equipment.
Risks and complications
OVE and OVH carry similar intraoperative risks including hemorrhage, inadvertent ureteral ligation, and incomplete removal of ovarian tissue. As discussed, there is the potential for less tissue trauma when performing an OVE because the uterine tissues are minimally manipulated. The more cranial location of the incision also improves visualization of the ovary, potentially decreasing the risk of postoperative ovarian remnant syndrome.
Potential long-term risks of spaying are well established and include urinary incontinence, decreased metabolism, and/or a predisposition to various joint conditions such as hip dysplasia, elbow dysplasia, and/or cruciate ligament disease. The incidence of these complications is likely equal for OVH and OVE procedures; however, existing literature is lacking. Early spaying at less than 6 months of age may be associated with an increased incidence of urinary incontinence and joint disorders.8 Additionally, heavier dogs with a projected adult weight of more than 25 kg may be at a higher risk of developing urinary incontinence if spayed earlier in their first year of life.9 There is a significant amount of breed variation for the development of orthopedic disease and urinary incontinence at different ages.10 The decision to delay performing a spay must be weighed against the increased likelihood of developing mammary cancer with consecutive heat cycles.
A common misconception is that performing an OVE increases the risk of developing a pyometra compared with an OVH as the uterine tissues remain present. Although the exact pathophysiology of pyometra formation is not completely understood, progesterone is known to play a key role. By removing the ovarian tissue, the source of endogenous progesterone is eliminated; therefore, a pyometra should not occur. One study evaluated 141 ovariectomized dogs over the course of 6 to 11 years and none developed a pyometra.11 It is important to note that a pyometra can still develop in an ovariectomized dog if there is exposure to exogenous estrogens, which is commonly found in topical hormonal replacement therapies used by menopausal women. Likewise, pyometras can occur in a similar manner in an ovariohysterectomized dog if all uterine tissue is not removed, which is uncommonly achieved in OVH procedures.12
Conclusion
There is no current consensus among veterinary surgeons on the preferred sterilization procedure in dogs. Both OVE and OVH are appropriate spay techniques for apparently healthy females. If uterine pathology is present, an OVH should be performed. Given the lack of advantages to removing the uterus in clinically normal dogs and the potential advantages of an OVE as discussed, OVE procedures may be more readily performed in the future.
Michael Cali, DVM, is a 2021 graduate of St. George’s University School of Veterinary Medicine in Grenada, West Indies, and received clinical training at the University of Florida in Gainesville. His internships include Auburn University in Alabama, mentored by Katelyn Hlusko, DVM DACVS-SA.
References
1. Charlesworth TM, Sanchez FT. A comparison of the rates of postoperative complications between dogs undergoing laparoscopic and open ovariectomy. J Small Anim Pract. 2019;60(4):218-222. doi:10.1111/jsap.12993
2. DeTora M, McCarthy RJ. Ovariohysterectomy versus ovariectomy for elective sterilization of female dogs and cats: is removal of the uterus necessary? J Am Vet Med Assoc. 2011;239(11):1409-1412. doi:10.2460/javma.239.11.1409
3. Davidson EB, Moll HD, Payton ME. Comparison of laparoscopic ovariohysterectomy and ovariohysterectomy in dogs. Vet Surg. 2004;33(1): 62-69. doi:10.1111/j.1532-950x.2004.04003.x
4. Hancock RB, Lanz OI, Waldron DR, Duncan RB, Broadstone RV, Hendrix PK. Comparison of postoperative pain after ovariohysterectomy by harmonic scalpel-assisted laparoscopy compared with median celiotomy and ligation in dogs. Vet Surg. 2005;34(3):273-282. doi:10.1111/j.1532-950x.2005.00041.x
5. Devitt CM, Cox RE, Hailey JJ. Duration, complications, stress, and pain of open ovariohysterectomy versus a simple method of laparoscopic-assisted ovariohysterectomy in dogs. J Am Vet Med Assoc. 2005;227(6):921-927. doi:10.2460/javma.2005.227.921
6. Johnston SA, Tobias KM. Veterinary Surgery: Small Animal. Elsevier; 2018.
7. Corriveau KM, Giuffrida MA, Mayhew PD, Runge JJ. Outcome of laparoscopic ovariectomy and laparoscopic-assisted ovariohysterectomy in dogs: 278 cases (2003-2013). J Am Vet Med Assoc. 2017;251(4):443-450. doi:10.2460/javma.251.4.443
8. Pegram C, Brodbelt DC, Church DB, et al. Associations between neutering and early-onset urinary incontinence in UK bitches under primary veterinary care. J Small Anim Pract. 2019;60(12):723-733. doi:10.1111/jsap.13072
9. Byron JK, Taylor KH, Phillips GS, Stahl MS. Urethral sphincter mechanism incompetence in 163 neutered female dogs: diagnosis, treatment, and relationship of weight and age at neuter to development of disease. J Vet Intern Med. 2017;31(2):442-448. doi:10.1111/jvim.14678
10. Hart BL, Hart LA, Thigpen AP, Willits NH. Assisting decision-making on age of neutering for 35 breeds of dogs: associated joint disorders, cancers, and urinary incontinence. Front Vet Sci. 2020;7:388. doi:10.3389/fvets.2020.00388
11. Okkens AC, Kooistra HS, Nickel RF. Comparison of long-term effects of ovariectomy versus ovariohysterectomy in bitches. J Reprod Fertil Suppl. 1997;51:227-231. PMID:9404289
12. Ivaldi F, Ogdon C, Khan FA. A rare case of vulvar discharge associated with exogenous oestrogen exposure in a spayed Weimaraner bitch. Vet Med Sci. 2022;8(5):1872-1876. doi:10.1002/vms3.860















Newsletter
From exam room tips to practice management insights, get trusted veterinary news delivered straight to your inbox—subscribe to dvm360.















