The vestibular cat (Proceedings)
The peripheral vestibular system connects directly with the central nervous system for control of posture and eye movements.
The peripheral vestibular system connects directly with the central nervous system for control of posture and eye movements. Any neuroanatomic disruption to the peripheral and central components will manifest in clinical signs of vestibular dysfunction.
Anatomy
Peripheral pathways: (Labyrinths)
The peripheral components of the vestibular system are enclosed within the vestibule of the inner ear, hence the name. Receptors for the vestibulocochlear system are contained within a membranous labyrinth that is encased within a bony labyrinth (semicircular canal, vestibule and cochlea). The membranous labyrinth is composed of the cochlear duct, three semicircular ducts, and the otolithic organs (utricle and saccule). The cochlear duct contains the major sensory area for hearing, the organ of Corti. The semicircular ducts, utricle and saccule contain sensory areas for controlling equilibrium. Perilymph, similar in constituency to cerebrospinal fluid (CSF), separates the boney and membranous labyrinths. The membranous labyrinth contains the fluid endolymph. Endolymph provides a medium by which the receptors within the semicircular ducts and otolithic organs can detect changes in head position.
Receptors detecting angular acceleration and head rotation are located within the crista ampullaris contained in the ampulla of each semicircular duct. The vestibular nerve transmits the appropriate signal for rate and direction of rotation to the central nervous system. Receptors detecting static head orientation and linear acceleration lie within the sensory area (maculae) of the utricle and saccule. The macula of the utricle lies in the horizontal plane and is important for detecting equilibrium changes in the upright position. The macula of the saccule lies in the vertical plane and detects equilibrium changes in the recumbent position. Differences in hair cell patterns within the macula allow for appropriate signal transduction concerning head orientation with respect to gravity and linear acceleration (primarily the utricle).
Central pathways: (Brainstem)
Vestibular neurons are bipolar with cell bodies located in the internal acoustic meatus of the petrosal bone. The vestibular nerve enters the brainstem at the level of the rostral medulla and caudal cerebellar peduncle in proximity to CN V and CN VII and primarily synapses with the vestibular nuclei. The central or brainstem portion of the vestibular system bilaterally consists of four vestibular nuclei (rostral, caudal, medial and lateral) that also receive input from the spinal cord and cerebellum. These nuclei have UMN projections to the spinal cord, reticular formation of the brainstem, CN nuclei III, IV, and VI, and cerebellum. The cerebellum functions closely with the vestibular system to control equilibrium during rapid changes of movement.
Neurologic examination findings
An animal with vestibular disease manifests abnormalities in eye position/movement, in head and body position and voluntary motor movements. The purpose of the neurologic examination is to determine the neuroanatomic localization of the vestibular disease i.e. peripheral vs. central disease. This is important because central involvement more commonly has a guarded prognosis and the diagnostic approach will differ. The abnormal neurologic examination findings are summarized below:
Mentation
- Peripheral: usually alert, disoriented
- Central: Usually abnormal - disoriented, depressed/obtunded
Head tilt
Presence of a head tilt obviously indicates vestibular dysfunction and an asymmetric disease process. The head tilt may vary in severity and may be a residual deficit with resolution of the disease process. In subtle cases, blindfolding the animal may accentuate the tilt.
- Peripheral: head tilt ipsilateral to lesion
- Central: head tilt ipsilateral or contralateral to lesion
Head turn
A head turn to the side of the lesion indicates unilateral disease. If associated with a head tilt, the yaw is vestibular in origin. (a turn without a head tilt the lesion may be forebrain - aversive syndrome)
Circling/leaning/rolling/falling
These findings indicate asymmetric vestibular dysfunction usually to the side of the lesion. Severe cases of unilateral vestibular disease often roll and fall. Circling usually is tight (wide circles more common with forebrain disease). The animal is driven in one direction due to an imbalance of input/output to/from the vestibular nuclei. Usually accompanied by decreased in ipsilateral extensor tone, lack of inhibition of ipsilateral flexor tone and increased in contralateral extensor tone. Severe leaning/rolling/falling is more commonly associated with peripheral vestibular disease. Circling also may be a clinical sign for the animal trying to maintain a sense of equilibrium.
Abnormal eye movements
The vestibular system provides the sensory input for motor outputs from CN nuclei III, IV, and VI to control normal eye movements with regard to changes in head position. The ascending MLF pathway provides the central connection to the CN nuclei. Strabismus is defined as abnormal eye position with stationary and change of head positions. Animals with vestibular dysfunction often have a ventrolateral strabismus ipsilateral to the lesion and elicited on dorsoflexion of the neck. Nystagmus defines eye movement. In normal animals, as the head is turned to one side slow movements occur to the opposite side followed by a quick phase or jerk of the nystagmus toward (ipsilateral) the side of the head turn (vestibule-ocular reflex or physiologic nystagmus). The slow phase also is known as the doll(s eye test and the fast phase is known as the oculocephalic reflex. Lagging of the fast phase or dysconjugate eye movements indicate vestibular dysfunction. Presence of spontaneous nystagmus indicates vestibular dysfunction. Imbalance in inputs to the vestibular nuclei may lead to the perception of head rotation of the normal side; thereby causing the eyes move in the opposite direction of the perceived rotation (slow phase toward the lesion) followed by a quick reset (fast phase away from the lesion). Positional induced nystagmus also indicates vestibular dysfunction. This can be elicited by rapid turning of the head from side to side, tilting the nose in a vertical direction or turning the animal upside down. An animal with vestibular disease decompensates and spontaneous nystagmus is elicited. Central vestibular disease should be highly considered if the direction of nystagmus is vertical or changes with a change in head position.
- Peripheral: horizontal or rotary nystagmus
- Central: horizontal, rotary or vertical nystagmus; fast phase direction variable; direction may change
Other cranial nerve deficits
Cranial nerve VII deficits and Horner's syndrome (sympathetic n. deficit) can occur concurrently in clinical signs of peripheral vestibular disease involving the inner ear (petrosal bone) and middle ear, respectively. Other CN deficits (CN V, IX, X, XI, XII) ipsilateral to lesion indicate central vestibular disease.


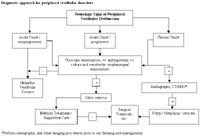
Diagnostic approach for peripheral vestibular disorders
Proprioceptive/sensory and motor deficits
Postural reaction testing can elicit evidence of limb paresis which indicates central vestibular disease. Conscious proprioceptive deficits indicate a disruption of the sensory pathways. Hopping, wheelbarrow and extensor postural thrust reactions require both the sensory (vestibular) and motor pathways to be intact. Postural reaction deficits occur ipsilateral to the lesion in central disease. If the clinical signs of vestibular disease are severe, postural reactions can be difficult to interpret. Usually an animal with peripheral vestibular disease has good strength associated voluntary motor movement.
- Peripheral: none
- Central: ipsilateral postural reaction deficits
Note: Animals with bilateral vestibular disease usually show a crouched posture, wide head excursions, wide base stance and decrease or absence in physiologic nystagmus when turning the head from side to side.



Summary of peripheral vestibular disorders
Note: Paradoxical vestibular disease is a form of central vestibular disease with clinical signs (head tilt, nystagmus) lateralized opposite of what one would expect with unilateral vestibular disease. Paradoxical syndromes are caused by lesions involving the rostral and medial vestibular nuclei, caudal cerebellar peduncles, nodulus of the cerebellum or the dorsal nerve roots of cervical nerves 1, 2, and 3.



Diagnostic approach for central vestibular disorders
Differential diagnosis, diagnostic testing and treatment of peripheral and central vestibular disorders
A thorough history and physical and neurologic examinations will assist in consideration of differential diagnoses (DAMNITV), diagnostic testing procedures and treatment plans. Disease processes of acute onset commonly include nutritional, idiopathic, inflammatory, toxic, traumatic and vascular disorders. Chronic disease processes include degenerative, inflammatory/ infectious, polyneuropathies, neoplastic and toxic disorders. Diagnostic procedures that evaluate for labyrinth pathology include: otoscopic examination, bulla radiographs, computed tomography, brain stem auditory evoked response (BAER) testing and myringotomy (puncture a hole in the tympanic membrane, collect fluid for cytology and culture). Wave I of the BAER is used to assess concurrent sensorineural deafness and waves II-V is used to assess central conduction abnormalities. Diagnostic procedures for central vestibular disorders evaluate for brainstem pathology. Magnetic resonance imaging (MRI) is used to diagnose structural brainstem disease such as neoplasia and some inflammatory disorders. Computed tomography also is useful; however, in small animals such as the cat bone artifact in the caudal fossa can interfere with visualization of subtle brainstem lesions. Cerebrospinal fluid analysis detects evidence of inflammatory disease.



Summary of central vestibular disorders