Transfusion support of the bleeding patient: Part I (Proceedings)
Whole blood can be stored or processed into one or more of the following components: red blood cells, platelets, plasma, and cryoprecipitate.
Whole blood can be stored or processed into one or more of the following components: red blood cells, platelets, plasma, and cryoprecipitate. The goal in veterinary transfusion medicine, however, is to limit whole blood transfusion and to use component therapy whenever possible. Blood components permit specific replacement therapy for specific disorders, reduce the number of transfusion reactions as a result of diminished exposure to foreign material, and decrease the amount of time needed to transfuse. Most importantly, appropriate therapeutic use of blood components increases the number of patients who benefit from this limited resource. Certain disease states will require replacement of one or any combination of components, and the component(s) chosen will depend on the crisis at hand.
Oxygen support
Oxygen transport is the main function of red blood cells (RBC), and it occurs mostly through the work of hemoglobin, a protein carried in the erythrocyte itself. Hemoglobin is composed of four polypeptide chains, each of which contains a single atom of iron that is capable of binding oxygen. Hemoglobin picks up oxygen in the lungs and transports it to where it is being released to organs and tissues. The extent to which hemoglobin binds oxygen is dependent on several factors, including the partial pressure of oxygen in the blood (PO2), pH, temperature, and (in dogs but not cats) the concentration of 2,3-DPG, a RBC metabolite that facilitates unloading of oxygen from hemoglobin to tissues. When blood hemoglobin content is low, such as in anemia, or if hemoglobin is not oxygenated in the lungs, such as with cardiopulmonary diseases, tissue hypoxia ensues. It is important to understand that without hemoglobin, very little oxygen is transported in blood. When the body can no longer compensate for the decreased oxygen availability, oxygen-carrying support must be instituted.
Allogeneic transfusion
Transfusion of RBC through whole blood (WB) or packed red blood cells (pRBCs) is typically used to augment oxygen-carrying capacity in patients with low packed cell volume (PCV). Nearly all oxygen contained in blood is carried by hemoglobin; therefore, RBC transfusions increase the oxygen-carrying capacity of the anemic patient, and thus can reverse inadequate delivery of oxygen to tissues. A "transfusion trigger", the packed cell volume (PCV) at which a red blood cell transfusion is administered, has not been clearly defined in human or veterinary medicine. The point at which a blood transfusion is necessary is based on the summation of clinical assessment and laboratory findings. A PCV of less than 15-20% is often considered a threshold at which to provide transfusion support, particularly in ill patients or patients undergoing surgery or other major medical interventions. Low PCV alone, however, is an inadequate parameter for RBC transfusion since there are so many additional factors (e.g., cardiac output and oxygen consumption) involved in tissue oxygenation in each individual patient. Tachycardia, poor pulse quality, pallor, lethargy, weakness, and decreased appetite are important clinical signs that may indicate that a patient is in need of additional oxygen-carrying support.
Whole blood
Initial collection from a donor yields fresh whole blood (FWB) and is defined as FWB for up to 8 hours after collection. FWB provides red blood cells, white blood cells, platelets, plasma proteins, and coagulation factors. Certain components in blood are more fragile than others and will become less effective with time and ambient temperature change. For example, platelet efficacy becomes questionable once whole blood is refrigerated. In order to achieve full benefit of all components when needed, FWB should be administered immediately following collection.
FWB is used in actively bleeding, anemic animals with thrombocytopenia/thrombopathia, anemia with coagulopathies and massive hemorrhage. In cases of severe hemorrhage, administration of all components may be necessary to support the patient. Massive hemorrhage is defined as a loss approaching or exceeding one total blood volume within a 24-hour period.
Following collection, whole blood must be processed into components or at least refrigerated at 1-6°C within 8 hours. After 24-hour storage of whole blood, platelet function is lost and the concentration of labile coagulation factors decreases. The product is then defined as stored whole blood (SWB) and provides RBC and plasma proteins (albumin, globulins). The length of time a unit of WB can be stored under refrigeration is dependent on the anticoagulant-preservative solution used in collection. With the advantages in the use of blood components so well documented in both human and veterinary medicine and the improved availability of these products as a result of commercial blood banks, the use of WB is no longer considered the treatment of choice. However, SWB can be used in patients that require intravascular volume expansion as well as oxygen-carrying support, albumin or coagulation factors. The use of WB, fresh or stored, is not recommended in severe chronic anemia. Chronically anemic patients most often have increased their plasma volume to maintain a normovolemic state. Rapid administration of WB may expose these patients to the risk of volume overload, especially in patients with preexisting cardiac disease or renal compromise.
Packed red blood cells
Packed red blood cells (pRBC) can be harvested from a unit of WB following centrifugation at 4°C, and stored at 1-6°C for approximately one month (definitive storage time is determined by the anticoagulant-preservative solution used in collection). Packed RBC is the component of choice for increasing red cell mass and oxygen transport in the anemic patient. Decreased red cell mass may be caused by decreased bone marrow production, increased destruction, or surgical or traumatic bleeding. Although it seems logical that blood loss should be replaced with whole blood, replacing blood volume with pRBC and crystalloid or colloid solutions adequately treats most blood loss in actively bleeding animals. This is often adequate therapy for the majority of acutely bleeding patients. Transfusion of pRBC is not recommended in patients who are well compensated for their anemia (e.g., chronic renal failure). The decision to perform red cell transfusion should never be based solely on hematocrit or hemoglobin levels. Patients should be properly evaluated and pRBC administration based primarily on clinical status (e.g., tachycardia, poor pulse quality, lethargy).
Alternative therapies
The shortage of banked blood products in veterinary medicine and the ever-expanding risk of blood incompatibilities and infectious disease transmission sparked interest in developing safe and effective alternatives to red blood cell transfusion. Transfusion alternatives are therapies that reduce the need for allogeneic transfusions. Options for specific pharmacologic intervention do exist (i.e., hemoglobin-based oxygen carrier solutions, iron, erythropoietin) and when indicated, should precede blood transfusion.
Hemoglobin-based oxygen carriers
Synthetic solutions that contain hemoglobin seem to be a logical substitute for RBC transfusion. The ideal red cell substitute would:
- augment oxygen delivery
- provide colloidal support
- be free of infectious agents
- be universally compatible and safe
- have room temperature storage and a long shelf life
- be readily available and reasonably priced
The quest for a hemoglobin-based oxygen-carrying solution (HBOC) led to the development of Oxyglobin®, an alternative for delivering oxygen to tissues. Currently, Oxyglobin® is available at a limited production rate.
Oxyglobin® (Biopure, Cambridge, MA) is a solution of purified, polymerized bovine hemoglobin in a modified lactated Ringer's solution. Under normal circumstances, hemoglobin in RBCs carries 98% of the circulating oxygen, while only 2% is carried in plasma. When Oxyglobin® is administered, it is the plasma hemoglobin concentration that is increased. It may be more effective than blood at delivering oxygen to tissues because it is carried in the plasma and offloads oxygen more readily than RBC. Its oxygen affinity is regulated by physiologic chloride concentration, not 2,3-DPG. In addition to providing oxygen-carrying support, Oxyglobin® also has a strong colloidal effect, which can be useful in patients who are hypovolemic as well as anemic. Its colloid effects, however, may be associated with circulatory overload in normovolemic and cardiac-diseased animals.
The volume of Oxyglobin® to be delivered depends on the patient's degree of anemia and underlying disease. The recommended dosage is 10-30 ml/kg intravenously; however, it's duration of effect is dose dependent:

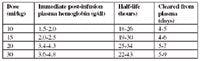
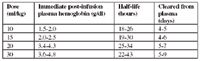
At these recommended dosages, the complications associated with volume expansion are minimized as longs as the volume status of the patient is such that colloidal solutions can be tolerated.
The best monitoring parameters in the anemic patient are physical examination findings, particularly respiratory and cardiovascular status, as well as hemoglobin concentration. Patients receiving Oxyglobin® require measurement of total (RBC and plasma) and/or plasma hemoglobin rather than PCV to assess how much of an impact has been made on oxygen-carrying support. For example, in a patient with a total hemoglobin concentration of 7 g/dl following administration of Oxyglobin®, the oxygen-carrying capacity of blood is approximately that of a packed cell volume of 21% (hemoglobin X 3 = PCV). In this patient, if the PCV is 3%, than a PCV equivalent of 18% is due to Oxyglobin.
Side effects can occur with administration of Oxyglobin®, including discoloration of the mucous membranes and sclera, increased central venous pressure, pulmonary edema, vomiting, and diarrhea. Following infusion of Oxyglobin®, the patient's serum will appear red, resulting in artifactual increases or decreases in the results of some serum chemistry tests (dependent on type of analyzer and reagents used). Complete blood count (CBC) results will be valid except for an increase in two RBC indices: mean cell hemoglobin (MCH) and mean cell hemoglobin concentration (MCHC). Total solids measurement will increase due to increased plasma protein in the form of hemoglobin. Oxyglobin® does not have an affect on hemostatic function testing (e.g., prothrombin time, partial thromboplastin time, platelet count, D-dimers). Given a small percentage of the hemoglobin solution is excreted by the kidneys, transient discoloration of the urine will occur and, therefore, urine dipstick measurements are inaccurate. Clearly, it is best to perform a CBC, serum chemistry, and urinalysis prior to the administration of Oxyglobin®.
The most significant limitation of Oxyglobin® in comparison to RBC transfusion is its relatively short half-life (30-40 hours at the recommended dose of 30 ml/kg) versus RBC survival of approximately 120 and 70 days in dogs and cats, respectively. Additionally, it is recommended as a single dose administration as antibodies to bovine hemoglobin may be produced after several days, although their significance is unknown. Due to the lack of RBC membranes in Oxyglobin®, crossmatching and blood typing are not necessary and hemolytic transfusion reactions are not a concern.
Iron
Iron is a mineral that is necessary for the synthesis of hemoglobin. Iron deficiency may result from insufficient dietary intake, impaired absorption, excessive demand, or chronic blood loss. By far, chronic blood loss is the most common cause of iron deficiency anemia. Chronic blood loss anemia is often the result of gastrointestinal bleeding, parasitism, chronically bleeding neoplasms, and chronic thrombocytopenia. A blood loss of 2-4 ml/day (1 to 2 mg of iron) is sufficient to cause this anemia in a smaller animal. Iron deficiency anemia develops gradually as iron stores are depleted and hemoglobin production is diminished.
Evaluation of the patient is based on clinical manifestations and laboratory tests. Microscopic study of a peripheral blood smear reveals that red blood cells have a hypochromic appearance due to their lack of hemoglobin. They are also microcytic, which may be appreciated by CBC. Iron stores are measured directly by bone marrow aspirate or biopsy, or indirectly by tests that measure serum iron, total iron-binding capacity, iron saturation and ferritin.



Erythropoietin
Erythropoietin (EPO) is a hormone produced by the kidney that promotes the formation of red blood cells in the bone marrow. Specialized cells in the kidney are sensitive to the oxygen content of the blood. When kidney hypoxia occurs, EPO production is increased, ultimately producing an increase in red cell mass and improvement in the oxygen-carrying capacity of blood.
Chronic renal disease in dogs and cats is often associated with anemia due to EPO deficiency. EPO therapy may be used for the long term management of anemia in these anemic patients. Although recombinant canine and feline EPO have been developed, the only commercially available form is recombinant human EPO. A major concern when using EPO is the formation of crossreacting antibodies which can lead to severe aplastic anemia. A dosage of 75 IU/kg is administered subcutaneously three times weekly initially, and then adjusted based on the patient's response to therapy. A relative decrease in EPO levels can also occur with chronic inflammatory disease, infectious disorders, and cancer. These patients may also benefit from EPO administration.
Summary
The lack of blood product availability, transmission of infectious disease and incompatibility reactions associated with allogeneic blood transfusion have made it a more complex therapeutic intervention in treating patients who require oxygen-carrying support. It is helpful to know that certain pharmacologic agents exist that can help improve oxygenation in specific anemic conditions without the inherent risks associated with RBC transfusions.
References available upon request














