Nausea, vomiting: First treat the underlying cause
Please provide a review of anti-emetic and prokinetic drugs - I am confused.
Please provide a review of anti-emetic and prokinetic drugs — I am confused.
Dr. David C. Twedt gave an excellent lecture on anti-emetics, prokin-etics and antacids at the 2008 American College of Veterinary Medical Forum in San Antonio. Here are some relevant points:
Vomiting and its management
Nausea and vomiting are common complaints and anti-emetics may play an important part in their management, but the primary objective should always be first to identify the underlying cause and if possible treat that primary disorder.
Anti-emetics are indicated when vomiting is severe, resulting in dehydration, electrolyte loss and acid-base disturbances, and for the prevention of motion sickness. Additionally, anti-emetics should be used for prevention of aspiration pneumonia, vomiting associated with radiation or chemotherapy, management of nausea resulting in inadequate nutritional intake and to enhance animal comfort.
Anti-emetics work either peripherally, centrally or in both areas. Vomiting is best defined as a reflex act initiated by stimulation of the conceptualized "vomiting center" in the brain's medulla oblongata. Activation of that center occurs through a humoral pathway initiated via blood-borne substances or through various peri-pheral neural pathways leading to the vomiting center.
Neural stimulation of the center arises through either afferent vagal, sympathetic, vestibular and cerebrocortical pathways. Activation of peripheral receptors found throughout the body can stimulate these neural pathways. Particularly important are receptors located throughout the abdominal viscera.
Central nervous system (CNS) disease may directly stimulate the vomiting center, such as direct extension of inflammatory stimuli, hydrocephalus or space-occupying lesions. The vomiting center is stimulated indirectly via a humoral pathway by activating the chemoreceptor trigger zone (CRTZ) located in the area postrema at the base of the fourth ventricle, an area devoid of a blood-brain barrier that allows exposure to chemical stimuli found in the circulation.
Blood-borne substances stimulating the CRTZ include certain drugs, uremic toxins, electrolytes, osmolars and acid-base disorders, as well as a number of metabolic derangements. There is evidence in the dog that vestibular stimulation passes through the CRTZ before activating the vomiting center. Motion sickness, inflammation of the labyrinth or lesions in the cerebellum results in vomiting via this pathway.
Anti-emetic drugs
Phenothiazine tranquilizers antagonize the stimulatory effects of dopamine. These drugs are reported to have weak anticholinergic and antihistaminic action. The potential side effects are hypotension from peripheral alpha-adrenergic blockade. Other effects include sedation and possibly seizures by lowering the seizure threshold. Chlorpromazine (0.5 mg/kg TID to QID given IV, IM, SC) is the most common anti-emetic from this class.
Antihistaminic drugs block both cholinergic and histamine receptor mediated transmission to the vomiting center arising from the vestibular system. These drugs generally are used for management of motion sickness or vestibular disease, but will cause some sedation. A common antihistamine used for this purpose is diphenhydramine (2-4 mg/kg TID given PO).
Anticholinergic drugs block cholinergic afferent pathways peripherally and pathways from the vestibular system leading to the emetic center. Drugs in this class tend to be poor anti-emetics and have the negative effect of altering gastrointestinal motility. Common drugs used in small animals include isopropamide (0.2-1.0 mg/kg BID given PO) and propantheline (0.25 mg/kg TID given PO).
Metoclopramide has anti-emetic effects through several mechanisms. At low doses it inhibits dopamine receptors and at higher doses inhibits serotonin receptors in the CRTZ. Cats are reported to have few CNS dopamine receptors and consequently metoclopramide may be a poor anti-emetic choice for them.

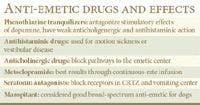

Anti-emetic drugs and effects
Metoclopramide is rapidly metabolized through the liver, and the best results are observed when given at continuous-rate infusion (0.01 to 0.02 mg/kg every hour or 1 to 2 mg/kg every 24 hours). At high doses it causes CNS excitement from dopamine antagonism. It also has effects on GI motility. Metoclopramide should be avoided in epileptics or in animals receiving other drugs that are likely to cause extrapyramidal reactions and should not be used with phenothiazine tranquilizers that can cause an additive effect.
Serotonin antagonists are effective at blocking serotonin receptors found peripherally, in the CRTZ and in the vomiting center. They are not very effective in relieving motion sickness. Common drugs used include ondansetron (0.1-1.0 mg/kg SID-BID given PO) and dolasetron (0.6 mg/kg given IV q 24 hours). They also are used for prevention of chemotherapy-induced vomiting. Another serotonin antagonist sometimes used in cats is mirtazepine (1.25-2.5 mg per cat PO once every three days). This drug not only is a serotonin antagonist, but also has an agonist effect that functions as an appetite stimulant.
Maropitant (1 mg/kg Q 24 hours given SQ or 2 mg/kg Q 24 hours given PO) is a neurokinin-1 antagonist that blocks receptors found in the emetic center, CRTZ and in peripheral afferent nerves.
Maropitant appears to be a good broad-spectrum anti-emetic approved for use in the dog. At higher doses (8 mg/kg given orally up to two consecutive days) it also prevents motion sickness. It is effective in preventing vomiting and nausea associated with chemotherapy and in management of parvovirus enteropathy and pancreatitis, as well as many other causes of vomiting.
It is not yet approved for use in cats, but some have used it in cats. Maropitant does not appear to effect GI motility. Because of its hepatic metabolism, it should be used with caution in animals that have significant hepatic dysfunction.
Prokinetic disorders and their management
Abnormal gastrointestinal motility generally is associated with megaesophagus, gastroesophageal reflux, gastric hypomotility, food hypersensitivity problems and chronic constipation. Dogs with megaesophagus do not respond to prokinetic agents because the esophagus in the dog is predominately skeletal muscle and does not respond to agents that effect visceral smooth muscle. However, gastric prokinetic agents are used to prevent gastroesophageal reflux.
Metoclopramide acts on both dopaminergic and serotoninergic receptors. The prokinetic effects are through cholinergic stimulation of the upper gastrointestinal tract mediated by antagonism at the receptors and activation of the serotonin receptors located in neural and non-neural tissues of the GI tract.
Metoclopramide increases the tone and amplitude of gastric contractions, relaxes the pyloric sphincter and increases peristalsis of the duodenum and proximal jejunum, resulting in accelerated gastric emptying and intestinal transit. It also increases the resting tone of the lower esophageal sphincter.
It is given orally at a dosage of 0.2-0.4 mg/kg a half-hour before meals three or four times a day. This drug is contraindicated in gastric-outflow obstructions, with concurrent phenothiazine or narcotic therapy, or if the animal has epilepsy.
Side-effects with metoclopramide are common, and include central nervous system abnormalities associated with hyperexcitability or depression. If side effects occur, the drug should be discontinued for 48 hours and then given at a lower dosage. This drug also has an anti-emetic effect attributed to its central anti-dopaminergic activity through actions at the CRTZ.
Cisapride is a promotility agent that is more potent than metoclopramide. The drug binds to serotonin receptors on enteric postganglionic cholinergic neurons and stimulates contraction of gastrointestinal smooth muscle. Cisapride increases lower esophageal sphincter pressure, improves gastric emptying and promotes increased motility of both the small and large intestine.
In cats, cisapride increases distal esophageal motility and has become an important prokinetic agent for management of feline megacolon. Cisapride was marketed as Propulsid, but was taken off the market because of induced cardiac arrhythmias referred to as "torsades de pointes" that resulted in sudden death in some people. Cisapride caused QT interval prolongation and slowing of cardiac repolarization as an explanation for the fatal arrhythmia. This abnormality has not been observed in dogs or cats.
Cisapride is now available only through compounding pharmacies. A recommended dose is 0.1 to 0.5 mg/kg BID to TID given 30 minutes before meals. Higher doses of 1 mg/kg may be required in some cases. Cats appear to tolerate a 2.5-mg dose without problems. Side effects include vomiting, diarrhea and abdominal discomfort. Cisapride should not be used with anticholinergic drugs because they will counteract cisapride's effect on motility. Cisapride may affect absorption of some drugs through increased GI motility. It has few, if any, effects as an anti-emetic.
Erythromycin is a novel prokinetic associated with frequent gastrointestinal side effects, including nausea and vomiting. The gastrointestinal effects occur from the drugs binding to motilin receptors in both cholinergic nerves and smooth muscle. In the dog, antral contractions are due to a cholinergic mechanism and in cats it is a smooth-muscle motilin agonist.
When given at very low sub-microbiological doses, erythromycin stimulates migrating motor complexes in the stomach. This motility occurs during the fasting state with an empty stomach, but studies have shown that, if given during feeding, it accelerates gastric emptying of food. It also increases lower esophageal sphincter pressure and may be useful in management of gastroesophageal reflux.
Erythromycin will increase colonic activity in the dog but not the cat. In dogs, a dose of 0.5 to 1 mg/kg given TID is the recommended prokinetic dose. Erythromycin also appears to be a better prokinetic drug than metoclopramide.
H2 receptor antagonists ranitidine (Zantac) and nizatidine (Axid) stimulate gastrointestinal motility in addition to their ability to inhibit gastric acid secretion. They function by inhibiting acetylcholinesterase activity and increasing the amount of acetylcholine available to smooth-muscle muscarinic-cholinergic receptors in the gastrointestinal tract.
When given at the normal anti-secretory doses, they also stimulate gastric contractions and accelerate gastric emptying. These drugs could be useful in the management of gastric ulceration with concurrent gastric hypomotility. Their relative potency as a prokinetic compared to the other drugs discussed is unknown but believed to be weaker.
Domperidone is both an anti-emetic and prokinetic agent not yet available in the United States. Domperidone is a peripheral and CRTZ dopamine receptor antagonist. It appears to be a better anti-emetic than prokinetic agent, having weak effects on GI motility. It has little effect on sustaining lower esophageal sphincter pressure, and gastric motility does not appear to be significantly enhanced during the fed state.
Antacid drugs
Oral antacids neutralize gastric acid to water and a neutral salt. Common antacids are bases of aluminum, magnesium or calcium. In addition to their acid-neutralizing ability, antacids decrease pepsin activity, bind to bile acids in the stomach and stimulate local prostaglandin production. Antacids are effective as long as they remain within the stomach and consequently must be given frequently. Antacids may interfere with the GI absorption of concurrently administered drugs and often cause constipation. Many OTC antacids are available.
Sucralfate (carafate) is a nonabsorbable compound containing aluminum hydroxide and sucrose octasulfate. When given orally, sucralfate forms a gel that has local effects on the gastrointestinal tract. It has a high affinity for ulcerated tissue, and will selectively bind with connective tissue in the ulcer, exerting a local protective role. It will inactivate pepsin, absorb bile acids, and the aluminum hydroxide portion has an acid-neutralizing effect. Studies have shown that this compound has a cytoprotective role thought to be caused by stimulating local tissue prostaglandins.
A dose of 1/4 to 1 gram three to four times a day is suggested, depending on animal size. The timing when given with other drugs has been a topic of debate, suggesting gastric acid is needed to dissolve the tablet, and that antacids should be given following sucralfate. That has not been proven in vivo and probably is of little significance; however, more important is the fact that sucralfate can bind to other drugs and inhibit their absorption. Sucralfate also is effective in treating esophagitis when given as a liquid.
H2-receptor antagonists such as cimetidine, ranitidine, famotidine and nizatidine are effective in reducing acid production by blocking the histamine receptor of the parietal cell. However, blocking only one of the three receptors on the parietal cell does not maximally inhibit all acid secretion. Some studies also suggest the H2-receptor antagonists may have benefits related to stimulation of local prostaglandin synthesis and thus a cytoprotective function.
The prophylactic value of H2-receptor antagonists to prevent gastric ulceration is at this time questionable, but they have been shown to be effective in healing ulceration. Cimetidine is given at 5-10 mg/kg QID given IV, IM, or PO. Ranitidine is more potent, has a longer half-life and is administered at 2 mg/kg TID and famotidine is dosed at 0.5 mg/kg BID or once daily. Cimetidine will alter hepatic biotransformation of certain drugs, and should be used with care in dogs with liver disease.
Proton-pump inhibitors (PPIs) block all acid production by the parietal cell by irreversibly binding the proton-transporting enzyme at the luminal surface of the cell. There is a delayed onset of action, but the duration of action is prolonged (24 hours or more) until new enzyme is produced. It is a potent acid blocker, effectively blocking all stimuli causing acid secretion (histamine, gastrin and acetylcholine). Omeprazole (Prilosec) is given at a dose of 0.7 mg/kg PO once a day. This drug is safe, with minimal side effects, but may compete with hepatic metabolism of some drugs. It is more effective in healing aspirin-induced ulcers than the H2 antagonists and may also have some gastroprotective effects, preventing gastric ulcer formation.
Omeprazole is recommended in animals with severe ulceration or those that fail to respond to traditional ulcer therapy, such as dogs with mastocytosis, gastrinomas or other causes of hypergastrinemias. PPIs are my choice when treating reflux esophagitis because the esophagus is easily damaged by gastric acid, and PPIs block all gastric acid-formation.
Prostaglandin E has potent anti-secretory effects as well as cytoprotective effects. The synthetic PGE misoprostol (Cytotec) is given at a dose of 2-5 mcg/kg QID. Misoprostol suppresses gastric acid secretion by inhibiting the activation of histamine-sensitive adenylate cyclase. The cytoprotective effects arise from stimulation of bicarbonate and mucus secretion, increased mucosal blood flow, decreased vascular permeability and increased epithelial cell renewal.
The main indication for misoprostol use is the prevention or treatment of gastric ulceration from NSAIDs. It is uncertain if misoprostol will improve healing of established gastric ulcers and apparently does not have distinct advantages over other antacids in treating ulcers not associated with NSAIDs. High doses cause diarrhea and abdominal cramping and should not be used in pregnant animals because it can cause abortion.
Dr. Hoskins is owner of Docu-Tech Services. He is a diplomate of the American College of Veterinary Internal Medicine with specialities in small animal pediatrics. He can be reached at (225) 955-3252, fax: (214) 242-2200 or e-mail: jdhoskins@mindspring.com.