Managing cats with facial pruritus
Previously, differentials of feline facial pruritus were discussed to include ectoparasites such as flea allergy, otodectes, Notoedres and cheyletiella, food allergy, atopy including possible food storage mite allergy and demodicosis. Less common differentials include infections such as dermatophytosis, viral, and bacterial pyoderma, Malassezia dermatitis, Pemphigus foliaceus (PF) and idiopathic facial dermatitis of the Persian cat. Clinically, many of these diseases appear similar including Pemphigus foliaceus and bacterial pyoderma which can be difficult to differentiate both clinically and histopathologically.
Previously, differentials of feline facial pruritus were discussed to include ectoparasites such as flea allergy, otodectes, Notoedres and cheyletiella, food allergy, atopy including possible food storage mite allergy and demodicosis. Less common differentials include infections such as dermatophytosis, viral, and bacterial pyoderma, Malassezia dermatitis, Pemphigus foliaceus (PF) and idiopathic facial dermatitis of the Persian cat. Clinically, many of these diseases appear similar including Pemphigus foliaceus and bacterial pyoderma which can be difficult to differentiate both clinically and histopathologically.



Alice JerominDVM, Dipl. ACVD
Dermatophytosis in cats may have many different presentations ranging from deep crusting lesions to miliary dermatitis to asymptomatic (Photo 1). It is thought to be more common in younger cats. We probably all should be performing more fungal cultures than we normally do. To rely on the Wood's light is to gain a false sense of security as more fungal species do not fluoresce than do. Also normal "scale" may light up under the Wood's light, yet an apple-green fluorescence is what is considered positive in dermatophytosis with Microsporum canis. Before using the Wood's light, it is important to allow the light to warm up for five to 10 minutes or a false negative result may occur. False negatives may also occur if iodine shampoos or topicals have been applied to the cat.
Other methods of diagnosing dermatophytosis include a trichogram (examination of hairs in oil under the microscope looking for fungal elements in the hair shaft), fungal culture using the Mackenzie technique of using a toothbrush to comb the cat for a five-minute period then implanting the hairs/bristles into the fungal culture medium, and skin biopsies with PAS or GMS stains. Fungal cultures should be kept in a dark, humid place and examined within a 10-day period. If positive, cultures should be submitted to the lab for identification to be sure dermatophytosis is present and not contaminants that may register a false positive. Therapies for dermatophytosis have been discussed at length in the past. Topical therapy alone to clinically affected focal areas can give a false sense of security as other areas of infection may be brewing, yet those areas are not being treated. I prefer systemic antifungals such as Fulvicin P/G 5mg/kg bid or Fulvicin U/F 30mg/lb bid or Itraconazole 5-10mg/kg/day along with weekly lime sulfur dips and treatment of the environment.
Dermatophytosis



Photo 1: Perioral dermatophytosis lesions in a cat. Remember some cats with dermatophytosis have no visible lesions.
Isolation of the affected cat is imperative. Liver enzymes need to be monitored with Itraconazole use as does complete blood counts with Griseofulvin for idiopathic pancytopenia particularly in FIV positive cats. Lufenuron has been published to be effective for dermatophytosis, yet personal experience suggests unreliable results. A series of two negative fungal cultures after treatment to ensure the patient's dermatophyte problem has resolved is important.
Bacterial pyoderma in the cat is certainly not as commonly diagnosed as in the dog, but is still a differential to consider in feline facial pruritus (Photo 2). Staphylococcus simulans is a normal staph resident of feline skin. Staphylococcus aureus has been identified in cats with pyoderma lesions. The patients are usually older cats and lesions may consist of epidermal collarettes or deep pyoderma with draining tracts. In the few cases reported, response to antibiotic therapy was important in making the diagnosis. Other diagnostics included skin biopsies which yielded a neutrophilic folliculitis, perifolliculitis or panniculitis. Certainly, ectoparasites and dermatophytosis must be ruled out before the diagnosis of a primary bacterial pyoderma can be made.
Bacterial pyoderma



Photo 2: Nonhealing bacterial pyoderma in an FIV-positive cat.
Viruses are important pathogens in respiratory infections in cats, yet rarely cause skin lesions. Viruses that can affect the skin in cats include feline poxvirus, herpes and calicivirus. These organisms can cause skin lesions as well as mucous membrane lesions. Skin biopsies and PCR testing can be helpful in achieving the diagnosis. Therapy consists of antibiotics, antivirals, lysine or interferon. In nonhealing skin wounds, the FeLV and FIV status of the patient should be determined.
Viruses



Photo 3: Idiopathic Facial Dermatitis of the Persian Cat. Note the excessive black material in the facial folds.
Malassezia infections in cats particularly affecting the facial folds may play an accompanying role in idiopathic facial dermatitis of the Persian cat (Photo 3). Affected cats have marked dark material deposited in the facial folds sometimes accompanied by erythema, ulceration, otitis and blepharitis. Malassezia yeast is sometimes isolated and treatment with antiyeast medications may help in some patients. Others may have secondary bacterial involvement, yet antibiotics may only produce partial resolution. Skin biopsies yield acanthosis, hydropic degeneration with dyskeratotic basal cells, sebaceous hyperplasia, with a mixed diffuse inflammation. Therapies have included systemic steroids, oral antifungals, hypoallergenic diets and oral cyclosporine. Unfortunately the etiology is unknown and the disease may be genetic. Included in Malassezia problems in cats is a yeast otitis/dermatitis particularly of the chin. It is possible that when the cat is grooming itself, it transfers yeast from the ears to the chin/lipfold area. Anti-yeast otic preparations along with oral ketoconazole or itraconazole may be helpful.
Malassezia infections


Photo 4: Crusting of the dorsal nose in a cat with pemphigus foliaceus.
Although most veterinarians consider pemphigus foliaceus (PF) to be rare, it is actually not uncommon to see this disease in cats with a facial dermatitis. Up to 80 percent with facial lesions of PF have been reported to be pruritic. Lesions may include crusting of the ear pinna, face, surrounding the nipples and nailbeds. Cats of any age may be affected (Photo 4). The patient may be febrile and have a leukocytosis, eosinophilia and/or mild anemia. On cytology of the lesions, acantholytic cells along with neutrophils or eosinophils may be present. In a referral practice, the history includes that the patient was initially responsive to steroid injections, and they are referred usually because of steroid tolerance. Skin biopsies are necessary to make the diagnosis, and it is helpful to have the patient as long off steroid as possible to obtain an accurate histopathological diagnosis (Photo 5). Skin biopsies of the crusts or if present, an intact pustule, should be submitted in 10 percent formalin along with a thorough history. Histopathological findings include subcorneal pustules composed of neutrophils, eosinophils and acantholytic cells and perivascular to interstitial inflammation consisting of neutrophils and mast cells (Photo 6). Pustules may span several follicular units. Fungal cultures must also be performed to rule out dermatophytosis since some fungal species produce acantholysis. Treatment of PF includes oral steroids such as prednisolone, methylprednisolone, triamcinolone or dexamethasone initially to get the disease into remission. Reduction or withdrawl of steroids is the ultimate goal since they may incite diabetes in the cat if used long term. The addition of Chlorambucil 0.2mg/kg qod may be needed in some patients who cannot be weaned off steroids.



Photo 5: Multifocal erythema/crusting on the face of the cat with pemiphigus foliaceaus.
With the use of Chlorambucil, complete blood counts need to be routinely checked for reduction of red blood cells, white blood cells and platelets. Other therapies include doxycycline 5 mg/kg bid which may have some activity in autoimmune disease and sunlight avoidance. Sun, at least in human autoimmune diseases, can cause a flareup of the disease. Unfortunately it is not known what triggers the autoimmune reaction of the adhesion between the epithelial cells which defines PF, but factors such as medications, vaccinations, insect bites or underlying neoplasia may play a role in some patients.
Pemphigus foliaceus
Again as with most derm problems, two identical in appearance patients may in fact (and usually do) have different diseases. In the case of the facially pruritic cat, ectoparasites are probably the first differential to rule out and a hunt for fleas, Cheyletiella, demodex or Notoedres should be undertaken. We all need to remember the liability with underdiagnosing dermatophytes-in fact my receptionist just adopted a kitten without any skin lesions two weeks ago, now the entire family has "ringworm" lesions and the cat has two to three fluorescing hairs on the muzzle. Not to say we need to fungal culture all kittens we examine, but at least explain the possibilities of any kitten developing dermatophytosis after a certain incubation period (unknown). Most of the differentials of feline facial pruritus can be ruled out by in office tests such as skin scrapings, combings, trichograms, fungal cultures, skin testing or ELISA testing, or food trials. In those patients where the inhouse tests are negative or inconclusive, skin biopsies are usually helpful in achieving the diagnosis.

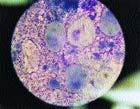
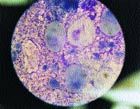
Photo 6: Cytology of an intact pustule of a cat with pemphigus foliaceus. The large mononuclear cells are acantholytic cells surrounded by neutrophils.















