Bad hips and bad knees, now what? (Proceedings)
A fairly recent study* showed that 32% of dogs referred to a surgeon for hip dysplasia treatment had, in fact, a torn ACL.
A fairly recent study* showed that 32% of dogs referred to a surgeon for hip dysplasia treatment had, in fact, a torn ACL.
Indeed, differentiating between a torn cruciate ligament and hip dysplasia can be tricky if not frustrating. Let's review the differences between the two conditions.
Cranial cruciate ligament tear
Severity of lameness depends on the severity of ligament disruption.
In stable partial tears, lameness can be subtle and noted only after periods of strenuous activity.
In complete tears, lameness will initially be severe and non weight-bearing. Then, moderate to severe weight-bearing lameness will occur.
In obvious cases, of course, a positive cranial drawer and a tibial thrust are the keys to diagnosing a cranial cruciate rupture. But what to do in less obvious cases?
Examination reveals various degrees of stifle pain with flexion and extension, variable crepitus, and possibly clicking associated with a meniscal tear.
In partial tears, a pain response is elicited when the joint is in full extension. In chronic cases, muscle atrophy is notable and peri-articular fibrosis (medial buttress) is evident on the medial side of the stifle. Medial buttress is almost pathognomonic for a cranial cruciate rupture. The only other condition that can present with medial buttress is a medial collateral ligament tear, which is usually seen with a deranged stifle, not a simple lameness.
Joint effusion is also a key finding: it can be palpated on the medial and lateral aspect of the patellar tendon.
Affected dogs have an abnormal "sit test," i.e. they sit with the affected leg extending out to the side, rather than sitting squarely (which they will do even with hip dysplasia). This is critical step in the evaluation. See below how this Lab does not want to flex his left knee.



In a partial tear, the cranial drawer may or may not be present. A sedated exam is needed to confirm the findings. MANY patients who don't seem to have a drawer while awake, suddenly have one once they are sedated and relaxed.
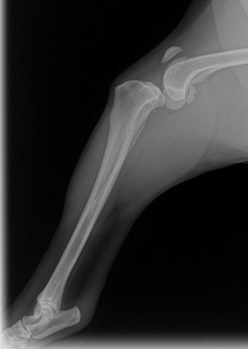
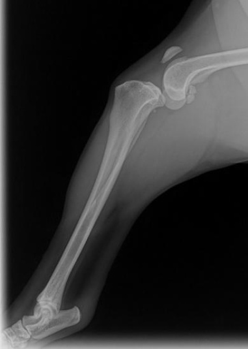
Radiographs are warranted in all cases to document stifle arthritis, to confirm pathology in challenging cases of partial tears, and to rule out other disorders (occasionally, we find a tumor).
The earliest and most consistent finding is the loss of infra-patellar fat pad shadow by a soft tissue opacity in the lateral view. This is consistent with effusion.
Caudal displacement of fat density located caudal to the joint capsule by a soft tissue opacity is also consistent with synovial distention.
In many cases, you can "see" the cranial tibial thrust on an X-ray. See below how subluxated the knee is.
Another consistent finding is osteophyte and/or enthesiophyte formation in the region of femoral trochlear ridges, tibial plateau, and at the base and apex of the patella.
Rupture of the contralateral cruciate ligament occurs in 37%-48% of dogs within 6-17 months of the initial diagnosis. However, rupture can be bilateral on presentation, often times giving them a “neurologic” crouched walk.
Hip dysplasia
Hip dysplasia causes joint inflammation and secondary osteoarthritis, which lead to variable degrees of pain. Clinical signs can vary from slight discomfort to severe acute or chronic pain. Although the disease onset has a linear progression over time, it can be divided into two forms.
The juvenile form typically affects dogs between 5 and 12 months of age. They present with unilateral or bilateral hind limb lameness, bunny hopping, and difficulty rising after rest, reluctance to walk, run, jump, or climb stairs, exercise intolerance, and pain on hip extension.
These clinical signs are the result of joint laxity.

The chronic form of hip dysplasia has a highly variable onset of clinical signs in old dogs. Pain is most often related to DJD and has a more chronic presentation. Clinical signs are similar to the juvenile form. Pain is elicited most notably during hip extension.
As the disease progresses, crepitus can be palpated with range of motion. A sedated exam followed by orthogonal radiographs will further support the diagnosis.
Hip dysplasia dogs have a normal "sit test," i.e. they sit with both legs flexed symmetrically.
Hip and knee
Of course, both conditions can be present at the same time. In the study mentioned above, 32% of dogs referred to a surgeon for hip dysplasia treatment had, in fact, a torn cranial cruciate ligament. Interestingly, 94% of those dogs with a cruciate tear had concurrent radiographic signs of hip dysplasia.
It is imperative to do a thorough orthopedic and neurologic exam to accurately localize the clinical signs to avoid inappropriate diagnosis and treatment.
My absolute best advice? If in doubt, repeat your entire exam under sedation. Let's go over the 7 magic benefits of sedation:
- Sedation allows you to check for cranial drawer, tibial thrust, Barden and Ortolani sign.
- Under light sedation, you may still notice a pain response: increased respiratory rate or pulling on the leg.
- Under heavy sedation, total relaxation allows you much better joint evaluation.
- Sedation allows you to tap the knee (arthrocentesis), which is an invaluable test.
Crudely, normal fluid = clear, tiny amount and viscous. Abnormal fluid = yellowish, large amount and watery.
- Sedation allows you to "block" a joint, with lidocaine and/or steroids.
- Sedation enables you to take X-rays in a perfect position (knee = TPLO position, with a quarter in the picture; hip = OFA style) without fighting or causing pain.
- Sedation allows you to focus and take your time without fighting with your patient and alienating your technicians.
Reference
M.Y. Powers et al. "Prevalence of cranial cruciate ligament rupture in a population of dogs with lameness previously attributed to hip dysplasia: 369 cases (1994-2003)." JAVMA 2005, Vol. 227, N 7, 1109-1111.










Episode 26: Hope for canine osteoarthritis sufferers
November 3rd 2020On this episode of The Vet Blast Podcast, Adam Christman, DVM, MBA, is joined by small animal surgeon and rehabilitation specialist, Kristin Kirkby Shaw, DVM, MS, PhD, CCRT, DACVS, DACVSMR, who discusses the rise in canine rehabilitation and her new resource for managing canine arthritis.
Listen



