10 top considerations in performing dental extraction procedures
Thoughtful scheduling and effective communication optimizes patient care. As a small animal practitioner, your time is scheduled for medicine, surgery, client consultation and dental procedures. The area of greatest difficulty in scheduling typically involves dental procedures.
Thoughtful scheduling and effective communication optimizes patient care. As a small animal practitioner, your time is scheduled for medicine, surgery, client consultation and dental procedures. The area of greatest difficulty in scheduling typically involves dental procedures.
I strongly encourage staff training to optimize scheduling. Comprehensive dental care is challenging to schedule due to the variability of dental pathology encountered. A well-planned schedule allows adequate time to provide optimal patient care. You can complete necessary procedures during a single anesthesia period and minimize complication by operating meticulously, without being "rushed". I also recommend that you have a realistic view of your procedural efficiency and level of skill. Do you have experience performing dental extractions? Are you prepared for complications, such as tooth fracture, jaw fracture or excessive hemorrhage? Is your dental operatory sufficiently equipped? Your staff needs to understand the nature and potential complexity of dental cases. The older cat presenting with a history of "pawing at the face" and no previous dental prophylaxis can be a very time consuming case. Do not over schedule oral surgery procedures if you hope to enjoy your day!
Effective client communication is essential in obtaining informed consent, and it minimizes risk of conflict or unhappiness. You must provide treatment options, cost estimates and potential risks before proceeding into dental procedures. Clients appreciate having options and involvement in deciding how to proceed in their pets' care. They particularly appreciate your caring attitude in referral to a specialist to save teeth. Strategic teeth, such as the canines and the carnassials (upper fourth premolar and lower molars) are especially important for function and should be saved if possible.


Photo 1: Severe periodontal disease is the most common indication for extractions.
Clients are very concerned about how oral surgery will affect their pet. They want to know how much pain their companion will experience, how their pet will eat and what he can eat. You will prove to the client you care by discussing these issues in treatment planning (pre-anesthesia exam), during the surgery (on the cell phone) and after the procedure. Effective communication creates "a win- win-win experience" for the patient, client and veterinarian.



Photo 2: Fractured teeth are sometimes too severe to repair.
1. Indications for extractions
There are many indications for dental extractions. The most common indication is severe periodontal disease (Photo 1).i These teeth may be mobile, are often painful and tend to be less difficult to extract. Your client needs to understand that these teeth are a detriment to their pet, and extraction will eliminate pain and chronic bacterial infection. Additional indications for extraction include teeth that are fractured (Photo 2), discolored, non-vital, in a fracture lineii, retained decidous or supernumary and for interceptive orthodontics (Photo 3), traumatic occlusion, dentigerous cysts and other dental pathology (internal or external resorption, or retained root fragments).


Photo 3: Interceptive orthodontics may require extractions.
2. The operatory should include a high-speed dental unit and intraoral radiography.
The dental operatory should be well organized and preferably isolated from distracting activities (such as the general treatment area). This allows the opportunity to focus on the dental procedure. A dental unit should include high and low-speed handpieces with an air-water syringe for irrigation.
The operatory should also include a dental radiograph machine (Photo 4). Survey skull (screened) films rarely are diagnostic for veterinary dentistry. I take intraoral radiographs before starting all dental extraction procedures. These radiographs are non-screened and of higher detail. They are useful for diagnosis, treatment planning, intra-operative orientation and to document completion of the procedure. Intraoral radiographs are particularly valuable for evaluation of the root anatomy. Curved (dilacerated), ankylosed, supernumary, fractured, retained root tips and other root anomalies may create tremendous difficulty and surgical complication, without radiographs. Radiographs exponentially improve your efficiency and effectiveness in dental extraction procedures!
Photo 4: Dental radiographs key to understanding root anatomy prior to an extraction.
3. Magnification and lighting improve visualization of the surgical field.
Dental extraction can be difficult due to a variety of reasons, including the inability to clearly see small structures. Feline roots undergoing resorption can be particularly challenging. Oral surgical procedures often are associated with moderate patient hemorrhage. Blood supply is excellent for healing however bleeding impairs visualization. The dental operatory must be equipped with appropriate lighting. Magnification offers tremendous advantages with visualization.
Remember: Your efficiency and effectiveness in performing dental extraction procedures is directly affected by your ability to see clearly!


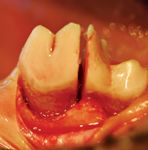
Photo 5: Multi-rooted teeth should be sectioned appropriately.
4. A variety of well-maintained instruments are essential for dental extractions.
Species and patient size variation necessitate a selection of instruments. Try using ophthalmic and other delicate instruments for oral surgery. I prefer Castrovejo needle holders and scissors, LaGrange scissors and small atraumatic tissue forceps. A selection of periosteal elevators, dental elevators, luxators and extraction forceps are essential. Root tip picks are particularly useful in retrieval of fractured root tips.
Surgical instruments must be sharp to optimize function and to minimize patient trauma. I strongly recommend a honing device for sharpening them. It is cost effective, very useful in a busy veterinary practice and will protect your investment in instruments. The technician can sharpen all dental and surgical instruments with this device. Your efficiency is improved in dental extraction procedures when using sharp instruments.



Photo 6: Schematics and models should be available for reference.
I prefer one of three scalpel blades mounted on a round scalpel handle for oral surgery (#15c, #15 and #11). The round handle offers improved control in making smooth curved incisions, particularly along the dental arcade. The gingiva is circumferentially incised around all teeth to be extracted.
5. Wide-based surgical flaps optimize blood supply and patient healing.
Mucogingival flaps are useful in performing dental extractions. The basic tenants of general surgery also apply to oral surgery. Surgical flaps should be wide based and orientated to maximize blood supply. Soft tissues are handled gently and maintained moist. Flaps provide adequate exposure to perform surgical extractions. I prefer a single mesial, vertical release incision for most flaps; however to allow for additional exposure, a second distal, vertical release incision may also be used. Diverging release incisions are preferred to maximize blood supply to the flap. Avoid neurovascular structures when making releasing incisions.
A periosteal elevator is used to elevate the flap from the alveolar bone and to protect it from injury during the extraction procedure. Be careful when elevating the firmly attached gingiva to avoid tissue damage (tearing).
6. Alveoplasty and sectioning of multi-rooted teeth simplify complete root removal.
Dental extraction is simplified when roots are removed individually. Multi-rooted teeth should be sectioned appropriately. I prefer using a 701 or 701L bur in a high-speed handpiece for tooth sectioning. Since roots are typically divergent, this technique will tremendously improve efficiency in dental extraction procedures. Schematic drawings, models or reference textbooks should be available for proper orientation.
Alveoplasty allows for greater exposure of the root and periodontal ligament (Photo 7). I prefer to use a #2 round bur in the high-speed handpiece to carefully remove 25 percent to 50 percent of lateral (buccal) bone. The quarter- or half-round bur may be used in the periodontal ligament space to help separate the tooth root from the alveolus.



Photo 7: Alveoplasty allows for greater exposure of the root and periodontal ligament.
Individual roots are circumferentially luxated. In luxation, the periodontal ligament is partially severed from the root and alveolar bone. The luxator is a sharp, thin instrument used as a wedge, it should not be rotated.iii The root is then elevated. I prefer to use a dental elevator that will maximize surface area in contact with the root (Photo 8). I can perform all extractions using my winged elevator set. For root elevation, gently twist or apply rotational force and hold, to gently tear the remaining periodontal ligament attachments. Luxation and elevation substantially "loosen" the root. It is then lifted out of the alveolus using an appropriately sized extraction forceps (Photo 9).



Photo 8: Consider using a dental elevator to maximize surface area in contact with the root.
The extraction forceps should not be used to forcefully "pull" the tooth root. Correctly sized instruments with gentle force will minimize risk of slippage and tooth fracture .



Photo 9: Extraction forceps lift the tooth out of the alveolus.
I always attempt to remove the entire root structure in cats and dogs, provided the procedure does not create unusual risk to the patient. If roots fracture and are not retrieved, the client must be notified and the patient followed radiographically for periapical disease. Pain, swelling, inflammation or draining tracks in areas with retained root tips must be addressed. These cases should be referred to a specialist if the operator lacks appropriate equipment, training or skill to correct the problem.
7. Instrument control and patient support avoids injury.
Dental extraction procedures involve controlled, gentle and deliberate force. I suggest you focus attention on instrument and patient stability to control force. The use of hand rests on stationary objects (such as the surgical table or the dental arcade) and finger stops with the instrument grasp will help avoid instrument slippage and potential injury (from deep penetration) to the patient or yourself. To create a finger stop, the forefinger of the hand holding the instrument should be placed a few millimeters above the alveolar crest from the working end of the instrument (Photo 10).



Photo 10: Use a fingerstop technique to avoid injury.
It is additionally helpful to support the patient's head with the opposite hand to control instrument force and to avoid patient movement.
8. Smooth the alveolar bone, curette and gently irrigate the alveolus to avoid blood clot disruption.
The alveolus should be smooth to allow for tension-free closure and to maximize patient comfort. A diamond bur may be used to smooth alveolar irregularities (Photo 11).
Photo 11: A diamond bur is used to smooth alveolar irregularities.
The alveolus should be visually and tactilely examined for fracture. Remove tooth remnants and bone fragments. Curettage of the alveolus will remove debris and aid in clot formation (Photo 12). The blood clot is important in the healing process. Gentle irrigation will help avoid clot disruption. Alveolar healing can be improved by packing osseogenic material into the alveolus.IV



Photo 12: Curettage of the alveolus to remove debris.
9. Suture all extraction sites with tension-free closure of flaps.
All gingival margins should be trimmed (or "freshened") and the connective tissue of the underside of the mucogingival flap is incised or "released" (Photo 13). These procedures allow for a tension-free closure and minimize dehiscence. The flap should be sutured in a simple interrupted pattern overlying bone. This maximizes patient comfort and avoids debris accumulation in the alveolus. I prefer 4-0 or 5-0 Monocryl suture; however Chromic catgut, Dexon, Maxon and Vicryl have also provided satisfactory results.


Photo 13: Gingival margins should be trimmed, and the connective tissue of the underside of the mucogingival flap incised.
10. Effective communication and patient re-evaluation creates a "win-win-win experience".
Written instructions should be sent home to summarize your home-care directions. I recommend that most surgical extraction patients receive analgesics for three to seven days post-operatively. Antibiotic therapy may be indicated in specific cases. Chlorhexadine solution rinses or zinc gluconate gels (Maxi/Guard) may additionally be used to help keep surgical sites clean. Hard-chewing objects are discouraged, and soft food is encouraged for 10 days. I recommend a two-week re-evaluation of the patient. If there is evidence of flap dehiscence, it should be repaired as soon as possible. Open extraction sites are uncomfortable for the pet and offer opportunity for infection. The recheck exam is a "value-added" step for the client and a "quality-control" procedure for your dental service. The patient, client and your practice will benefit in this experience, especially if you listen carefully, communicate effectively and provide optimal patient care.
Dr. Kressin, a Diplomate of the American Veterinary Dental College, operates a specialty dental and oral surgery service in Oshkosh and Milwaukee, Wis. He is a fellow of the Academy of Veterinary Dentistry.
i Harvey CE, Emily PP. Oral Surgery. In: Small Animal Dentistry. St Louis: Mosby, 1993: 313.
ii Schloss AJ, Manfra Marretta S: Prognostic factors affecting teeth in the line of mandibular fractures. J. Vet Dent 1990; 7:7-9.
iii Holmstrom S, Frost P and Eisner E. Exodontics. In: Veterinary Dental Techniques for the Small Animal Practitioner 2nd ed W.B. Saunders Co., 1998: 220-221.
iv Lobprise HB, Wiggs RB. Oral Surgery. In: Veterinarian's Companion for Dental Procedures. Lakewood, Co: AAHA Press, 2000: 82.

















